
A Disc Problem Isn't Always a Disc Problem
Your MRI is real. Your disc finding is real. The pain you feel when you bend, sit, or sleep wrong is absolutely real.
This is not a post telling you your disc isn't the issue, or that the imaging is meaningless, or that you should ignore what a radiologist saw on the scan.
It is a post about why so many people in Charlotte who have been told they have a bulging disc, a herniation, or degenerative disc disease end up back in pain after PT, after injections, and sometimes after surgery — and what changes when the actual mechanical problem gets addressed.
Think of Your Disc Like a Tire
A car tire is built to handle thousands of miles of normal load. Even good tires wear out eventually. But if your car is out of alignment — if one wheel is pulling, if the suspension is locked up, if the frame is twisted — that tire wears out years before it should. The tire isn't defective. It's getting hammered with load it was never supposed to carry.
Your lumbar discs work the same way. They are designed to handle compression. They are designed to absorb shock when you bend, lift, twist, and sit. Healthy discs do this for decades without issue.
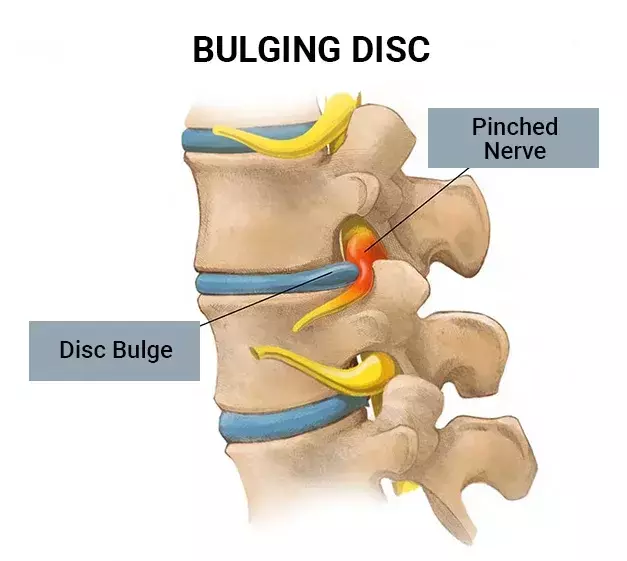
But when the structures around the disc — your hips, your hamstrings, your deep spinal stabilizers, your nerve pathways — get locked up by adhesion, the disc has to absorb load that should have been shared by the rest of the system. Year after year. Thousands of small movements. The disc starts to bulge, herniate, or degenerate not because it failed, but because it has been carrying weight that was never meant to be its job.
This is the part of the picture that imaging cannot show, and that most disc treatment never addresses.
What Adhesion Is and Why It Matters for Your Disc
Adhesion is dense, fibrous, scar-like tissue that builds up inside muscles, around nerves, and between joint structures over time. It forms from overuse, prolonged sitting, repetitive motion, and old injuries that never fully resolved. It glues tissue down that should slide and glide.
In a disc patient, adhesion almost always shows up in the same set of places:
-
The deep hip rotators (piriformis and the smaller external rotators) — when these are stuck, the hip can't extend properly, so every step transfers load to the lumbar spine
-
The hip flexors (psoas and iliacus) — when these are locked down, they pull the lumbar spine into hyperextension and compress the disc from the front
-
The hamstrings — when these are restricted, the pelvis can't rotate forward when you bend, so the lumbar spine has to flex more than it should
-
The deep spinal stabilizers themselves — when these are stuck, segments of the spine that should move stop moving, and the segments above and below take up the slack
-
The nerve pathways exiting the lumbar spine — when nerves get adhered to surrounding tissue, they amplify pain signals that a free nerve would tolerate
MRI cannot see any of this. It is not a defect in MRI technology — adhesion just doesn't have the density gradient that imaging is built to detect. So when a disc patient gets imaged, the disc finding is what shows up. The full story doesn't.
The Question Every Disc Patient Eventually Asks: Do I Need Surgery?
This is the elephant in the room and it deserves a direct answer.
Sometimes the answer is yes. There are clear cases where disc surgery is the right call:
-
Progressive neurological deficit (loss of strength, loss of bladder/bowel control)
-
Severe stenosis with cauda equina symptoms
-
Pain that has not responded to anything and is preventing basic function — and where surgical candidacy has been carefully assessed
Outside of those cases, surgery is much more often elective than patients are led to believe. We see it all the time: a disc bulge on imaging gets identified as the cause of pain, conservative care is tried for a few months, the conservative care doesn't address adhesion, the pain doesn't resolve, and surgery becomes the recommended next step.
Here is what we have learned from the post-surgical patients we treat: the surgery often does exactly what it was supposed to do. The disc material gets removed. The nerve gets decompressed. The structural finding on imaging is corrected. And the patient still hurts — sometimes worse than before.
Why? Because the adhesion that was loading the disc in the first place was never addressed. The structural problem was solved. The mechanical loading problem was not. And surgery itself adds new scar tissue that becomes another layer of restriction.
This is not an argument against disc surgery. It is an argument for finding out whether you can avoid it before you commit to it.
What Actually Predicts Whether You Can Avoid Surgery
After eight years of treating chronic disc patients in Charlotte, the patterns are consistent. Patients who can typically avoid surgery share these characteristics:
-
Pain has been present for more than three months but is not progressively worsening
-
Symptoms change with position — sitting makes it worse, walking helps, or vice versa
-
No loss of strength in the leg, no loss of bowel or bladder function, no severe night pain that wakes them every two hours
-
Pain pattern matches a tissue (sciatic nerve along the leg, glute and posterior thigh, lateral hip) — not a vague all-over ache
-
Movement testing reveals restrictions — straight leg raise is limited, hip extension is limited, lumbar flexion is limited — that improve with treatment
If those things are true for you, the odds of getting out of pain without surgery are high. Not guaranteed. But high enough that it is worth knowing before you sign the consent form.
Patients who genuinely need surgery have a different pattern — and we will tell you that, in your consultation, if that is what we see. We have referred patients out for surgical evaluation. It does happen. It is just much less common than the system makes it appear.
What Changes When the Adhesion Around Your Disc Gets Treated
The mechanic is straightforward. When the hip rotators, hamstrings, deep spinal stabilizers, and nerve pathways stop being stuck, three things happen:
Load gets shared. The disc stops absorbing the work that the rest of the system should have been doing. Compression decreases. Inflammation in and around the disc starts to settle.
Nerves stop being amplified. A nerve that was glued to surrounding tissue becomes free again. The same disc bulge that was producing severe symptoms can become almost asymptomatic, even though the bulge itself is unchanged.
Range of motion returns. You can bend. You can sit longer. You can sleep on your side again. The body stops protecting the disc through tension and starts trusting movement again.
None of this requires the disc itself to change. The bulge or herniation can stay exactly where it is on imaging. The pain can still resolve.
What the Work Actually Looks Like for a Disc Patient
Adhesion Release Methods (ARM) is the system we use. For disc cases, the visit-by-visit pattern is consistent.
Visit one is a 30-minute consultation. We take a detailed history of how your symptoms behave — when they're worse, when they're better, what triggered them, what has and hasn't worked, what your imaging shows. By the end, we can usually tell you whether adhesion is likely a major part of your case.
Visit two is a one-hour exam and first treatment. We do movement testing — the same provocative tests that change as adhesion gets released. We palpate the priority tissues. We treat the highest-priority structure for ten to fifteen minutes. Then we retest the same movement we treated. If the test improved, you feel it in the room. If it didn't, we know we're working on the wrong tissue and we change direction.
Visits three through twelve or so are focused treatment. Each visit follows the same loop: test, treat, retest. Most disc patients see meaningful symptom change between visits four and eight as the cumulative load on the disc keeps decreasing.
The endpoint isn't a number. It's a function. When you can do what you came to us to be able to do — sit through a workday, sleep through the night, lift your kids, get through a flight, run again — and the test improvements have stabilized, treatment is done. Most patients move into a maintenance schedule afterward so the adhesion doesn't rebuild.
What Your Specific Pattern Tells Us
Disc patients fall into a few common patterns. Yours probably looks like one of these:
Pain mostly with sitting and bending forward
This is the classic anterior disc-loading pattern. The disc gets compressed in flexion. Almost always involves significant hip flexor adhesion (psoas, iliacus) pulling the lumbar spine forward, and hamstring restriction preventing the pelvis from rotating. Highly responsive to ARM.
Pain that radiates into the glute, posterior thigh, or calf
Nerve involvement — usually the sciatic nerve or one of its branches getting amplified by adhesion in the hip rotators or hamstrings. Often labeled 'sciatica' but driven by the soft tissue, not the disc itself. Our condition page on sciatica and nerve entrapment covers this in detail.
Pain that's worse standing or walking, better sitting
This is more often a stenosis or extension-loading pattern. Adhesion in the deep spinal stabilizers and quadratus lumborum is usually present. ARM still helps significantly even when imaging shows stenosis, because the soft tissue around the narrowed canal can still be unloaded.
Pain that's been present since a surgery
Post-surgical disc pain is one of the most common presentations we see. The structural fix happened. The mechanical loading problem didn't. Surgical scar tissue itself becomes another adhesion site. Treatment is slower than for non-surgical cases — usually 16 to 24 visits — but the gains are real.
Pain in multiple body areas, with the disc being one of them
If your disc pain is part of a broader chronic pain picture across multiple regions, the disc may not be the right starting point. Our broader piece on chronic pain after multiple failed treatments lays out that situation.
Normal MRI but disc-like symptoms
More common than people realize. Adhesion produces back and leg pain that mimics disc pain even when imaging is clean. Here is the full breakdown of why a normal MRI does not rule out a real mechanical problem.
Specific Questions Disc Patients Ask
My MRI shows a 5mm bulge at L4-L5. Doesn't that mean the bulge is the problem?
Not on its own. Studies have shown that MRIs of pain-free adults find disc bulges in roughly 30 to 40 percent of people in their forties, and over half of people in their sixties. The bulge is a finding. Whether it is the cause of your pain depends on whether the surrounding tissue is loading it. In nearly every chronic case, the answer is yes — and removing that load is what changes things.
If I get an injection and feel better for a month, does that mean the disc is the problem?
It means the inflammation around the nerve was the immediate pain generator. That doesn't tell you what was creating the inflammation. Adhesion creating sustained mechanical load on the nerve and disc will keep producing inflammation long after each injection wears off. That's why injections often work for weeks and then stop working entirely.
Why do I feel a sharp twinge sometimes when I sneeze, cough, or strain?
Sudden pressure spikes (sneeze, cough, lifting, straining) momentarily compress the disc and can briefly aggravate a sensitized nerve. The fact that you have these spikes doesn't mean your disc is unstable or about to rupture. It usually means the nerve is in a sensitized state because of ongoing load — which is the thing ARM directly addresses.
My surgeon said the surgery went well and I should be fine. Why am I still in pain?
Because the surgery solved the structural problem (the bulge or compression) but not the mechanical loading problem (the adhesion that caused the structural problem in the first place). Plus, surgery itself creates new adhesion as the body heals. Post-surgical disc patients often need ARM more than non-surgical patients do.
Can I still exercise with a bulging disc?
Yes — and you should, in most cases. The question is what kind. Heavy spinal loading (deadlifts, squats, axial-loaded work) is risky if your disc is symptomatic. But low-impact movement, walking, and the kind of focused stabilization work we prescribe specifically build the capacity that protects the disc. Exercise is part of the answer; the wrong exercise can be part of the problem.
How is this different from chiropractic, PT, or massage?
Chiropractic adjusts joints. PT strengthens muscle. Massage reduces tone. None of them break down adhesion directly. ARM is hands-on, sustained, specific pressure on identified adhesions, with an immediate retest of function after every treatment. The retest is the part that doesn't exist in any other modality — you don't have to hope it worked.
What does this cost and how long does it take?
Costs and timelines are case-specific and we'll give you exact numbers in your consultation based on what we find. Average non-surgical disc cases run 12 to 16 visits over three to four months. Post-surgical cases run longer. We do not take insurance — pricing is transparent and based on results, not coded time.
If You're Still Trying to Decide What to Do Next
If you have a disc finding on imaging, if PT or injections haven't held, if you've been told surgery is the next step but you want to know whether you can avoid it — a consultation is the right next move.
We will take a full history, look at your imaging if you have it, do basic movement testing, and tell you honestly what we think. If we believe ARM can help, we will say so and explain how. If we believe surgery is the right call, we will say so and refer you out. Schedule a consultation with us at Resolve STS in SouthPark Charlotte.

Zac Breedlove
Contact Me
.jpg)
.jpg)